Introduction
Etiology of Testicular Torsion
The Epidemiology of Testicular Torsion
The Pathophysiology of Testicular Torsion
The History and Physical Manifestation of Testicular Torsion
Distinguishing Between Testicular Torsion and Appendage Torsion
The Treatment and Management of Testicular Torsion
References and Further reading
Testicular torsion is classified as an emergency condition. It occurs when this spermatic cord, from which the testicle is suspended, rotates and occupies a twisted orientation. This twisting prevents the testicle from receiving blood and causes sudden pain and swelling.
The tunica vaginalis, a pouch of serous membrane that covers the testes, is typically adhered to the posterolateral side of the testicle, and inside it, the spermatic cord is not able to move. If the attachment of the tunica vaginalis is strong, this enables the spermatic cord to twist inside, which subsequently leads to intravaginal torsion.
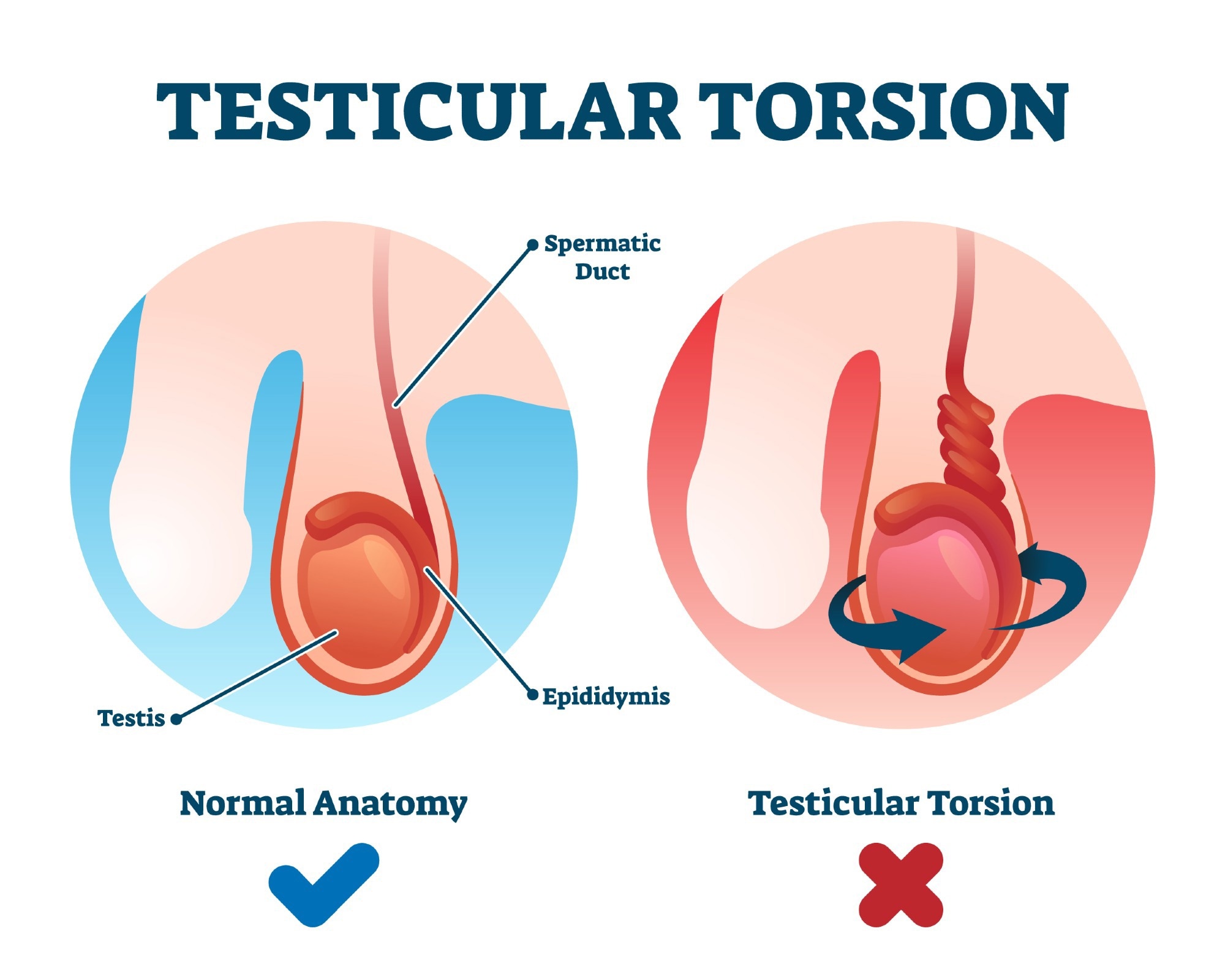
Image Credit: VectorMine/Shutterstock.com
Etiology of Testicular Torsion
Most cases of testicular torsion occur in young patients, that is, those under 25 years, and are typically caused by a congenital abnormality of the processus vaginalis, a blind-ended evagination of the abdominal wall that develops during fetal development.
Onset may be spontaneous because, as a result of exertion or comments, in very few cases, associated with trauma.
Neonates made develop extra vaginal torsion, by contrast. This occurs because the tunica vaginalis has not adhered to the gubernaculum, a ligament in the fetus that is attached at one end to the testes and the other to the scrotum. This occurrence may occur several weeks or months before birth.
Testicular torsion is also associated with the presidents of testicular malignancy in adults.
The Epidemiology of Testicular Torsion
In theory, testicular torsion can occur at any age and in the pre-or perinatal period. However, the majority of cases occur in adolescent males during periods of growth. The most common adverse outcome is testicular loss.
The Pathophysiology of Testicular Torsion
As a consequence of the testicle twisting around the spermatic cord, the flow of blood through the venous cavern of the spermatic cord is cut off. Consequently, the testicle becomes swollen, tender, and possibly red (erythematous). As the testicle undergoes further twisting, the blood supply through the artery is cut off, which exacerbates testicular ischemia and may eventually cause necrosis.
In most individuals suffering from testicular torsion, the testicle rotates between 90 and 100 degrees, and blood flow is subsequently compromised. Complete torsion is very rare and very quickly reduces the viability of the testes.
It is possible to salvage the testes if the torsion occurs for <8 hours. However, viability is rife if testicular torsion occurs for longer than 24 hours. Approximately 40% of people require testicular removal.
The History and Physical Manifestation of Testicular Torsion
Testicular torsion most commonly occurs abruptly and is associated with unilateral scrotal pain. The pain may be consistent or intermittent; however, it is not confined to a particular point in the testes. In addition, patients may demonstrate symptoms of nausea or vomiting which may or may not be associated with lower abdominal and groin (inguinal) pain. Alternatively, these forms of pain may be the dominant complaint as opposed to scrotal pain.
Regarding physical position, the testicle may be positioned abnormally, or transverse lie (that is, positioned horizontally), and may lie in a high position. As stated, the testicle may be swollen and red (erythematous). In addition, it may not produce the cremasteric reflex.
The cremasteric reflex is a superficial reflex found in human males that is elicited when the inner part of the thigh is stroked. In a normal response, the cremasteric muscle contract, which results in the scrotum being pulled on the testes.
However, the sensitivity of the cremasteric reflex is poor and may be reliable in young patients, particularly those that are <1 year of age.
Antibodies eBook
Image Credit: Yeexin Richelle/Shutterstock.com
Distinguishing Between Testicular Torsion and Appendage Torsion
Torsion of testicular appendages is more common than the torsion of the testicles; however, it is not as dangerous. During initial almost at, it can be distinguished from testicular torsion by maximum tenderness near the head of the epididymis or testes. Moreover, an isolated tender nodule and/ or a blue spot may appear on the testis.
The Treatment and Management of Testicular Torsion
Those who suffer any testicular torsion symptoms must seek urologic consultation immediately. This is because any delay in treatment can result in testicular necrosis and loss as a consequence of cut-off blood supply.
The typical window of opportunity for surgical intervention and successful salvage of the testicle is 6 hours from the onset of pain. Consequently, urologic surgery consultation at the point of the presentation can be a critical action even if confirmatory testing has not been conducted.
If conducted within six hours, the chance of salvages is approximately 90%. At 12 hours, the rate decreases to 50%, and at 24 hours, it reaches 10%. After 24 hours, the possibility of saving a testicle approaches 0 – however, there have been cases reported in which the testicle has been saved beyond 24 hours.
Detorsion of testicular torsion can be attempted if urological intervention is not immediately available. To achieve this, the affected testicle can be rotated in a medial to lateral direction, i.e., open book orientation, 180 degrees, and then evaluated for pain relief. If pain, however, is increased in the patient, a testicle may be rotated in the opposite direction.
To relieve pain, a patient may be given opioids.
In most cases, ultrasound can be used to evaluate whether or not blood flow has been returned at the site.
Overall, testicular torsion can occur at any age and even before birth. Treatment usually involves emergency surgery, and outcomes highly depend on the response time. If the testicle torsion is corrected within a six-hour window, testicular salvage is possible.
However, when blood flow has been cut off for longer than this, the risk of damage to the demitasse tickle increases and may ultimately result in a testicular loss period. Alternatively, several complications of testicular torsion may arise, which include infertility (although the effect of torsion on fertility is not yet understood), immunological theory (activation of the immune system to clean up damaged cells which produce anti testicular antibodies that crossed the blood testes barrier and damaged both the affected and contralateral testicle), microcirculation abnormalities, reperfusion injury (as seen in conditions of ischemia, as a consequence of prolonged periods of blood supply deprivation), sepsis and alongside psychological issues associated with losing a testicle (if testicular salvage is not possible).
References:
- Schick MA, Sternard BT. Testicular Torsion. [Updated 2021 Aug 2]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2021 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK448199/
- Naouar S, Braiek S, El Kamel R. (2017) Testicular torsion in undescended testis: A persistent challenge. Asian J Urol. doi: 10.1016/j.ajur.2016.05.007.
- Friedman AA, Palmer LS, Maizels M, et al. (2016) Pediatric acute scrotal pain: A guide to patient assessment and triage. J Pediatr Urol. doi: 10.1016/j.jpurol.2016.03.003.
- Tydeman C, Davenport K, Glancy D. (2010) Suspected testicular torsion – urological or general surgical emergency?. Ann R Coll Surg Engl. doi:10.1308/003588410X12771863937007.
- Howe AS, Vasudevan V, Kongnyuy M, et al. (2017) Degree of twisting and duration of symptoms are prognostic factors of testis salvage during episodes of testicular torsion. Transl Androl Urol. doi:10.21037/tau.2017.09.10.
Further Reading
- All Penis Content
- Penile Curvature – Peyronie’s Disease, Dupuytren’s Contracture
- Hypospadias outcomes
- Hypospadias
- Hypospadias Research
Last Updated: Mar 24, 2023

Written by
Hidaya Aliouche
Hidaya is a science communications enthusiast who has recently graduated and is embarking on a career in the science and medical copywriting. She has a B.Sc. in Biochemistry from The University of Manchester. She is passionate about writing and is particularly interested in microbiology, immunology, and biochemistry.
Source: Read Full Article