Scientists at the Centro Nacional de Investigaciones Cardiovasculares (CNIC) have designed an algorithm that provides a personalized estimate of cardiovascular risk in healthy middle-aged individuals based on a range of variables including age, blood pressure, diet, and blood and urines markers. The EN-PESA algorithm is an affordable tool for estimating the severity of subclinical atherosclerosis—characterized by the deposition of fatty substances in the arterial walls—especially in individuals at higher risk. The researchers conclude that EN-PESA will “help to personalize the estimation of cardiovascular risk, leading to tailored treatments and follow-up plans.”
The study, published today in The Journal of American College of Cardiology (JACC), forms part of the PESA-CNIC-SANTANDER partnership project, which is led by Dr. Valentín Fuster. The PESA study was launched in 2010 and was recently extended until 2030, and is one of the most important cardiovascular prevention studies in the world.
“Machine learning algorithms are set to revolutionize clinical practice in the coming years, impacting everything from diagnosis to prevention and treatment. More accurate risk quantification will allow highly precise, personalized risk estimates based on the totality of available information about each individual,” says Enrique Lara Pezzi, principal investigator on the current study and leader of the Molecular Regulation of Heart Disease laboratory at the CNIC.
The success of machine learning algorithms derives from the analysis and systematic processing of huge quantities of data collected from a large number of individuals. According to the Head of CNIC Bioinformatics Unit Dr. Fátima Sánchez Cabo, “PESA-CNIC-SANTANDER has been a pioneering study collecting large amounts of detailed phenotypical information from all participants of the study.”
Atherosclerosis is usually detected at advance stages, when it has already caused clinical events such as a heart attack or stroke. Treatment of atherosclerosis at this stage, after it has shown symptoms, is of limited success. A high proportion of surviving patients experience a decline in their quality of life, and the diminished patient health incurs increased costs for health systems. This is why it is so crucial to detect the disease at the earliest stages.
Since its launch in 2010, the PESA-CNIC-SANTANDER study has characterized more than 4000 parameters related to atherosclerosis. A central feature of the study is its use of advanced imaging techniques, and PESA-CNIC-SANTANDER also collects data on lifestyle parameters, biochemical and molecular markers, and the medical health of more than 4000 employees of Santander Bank who volunteered to participate in the study.
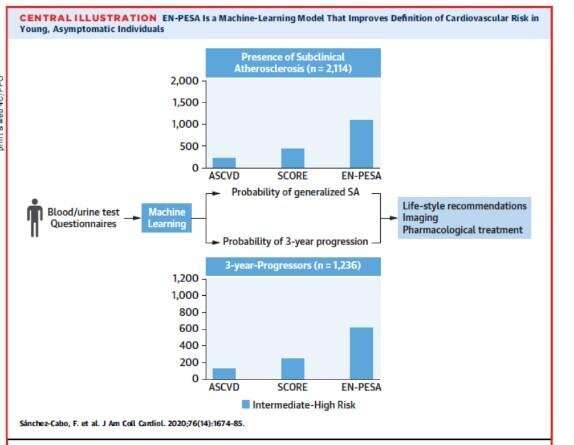
Sifting through this immense quantity of information, the CNIC algorithm identified a small set of variables that are easily measured in primary care centers. Dr. Xavier Rosselló, a CNIC researcher and cardiologist at Son Espaces university hospital in Mallorca, explained that these variables “provide an accurate prediction of the extent of subclinical atherosclerosis and disease progression in middle-aged individuals classed as being at low or intermediate risk according to established cardiovascular risk scales.”
The parameters include age, blood pressure, data collected in routine blood and urine analysis, and answers to dietary questionnaires.
Dr. Sánchez Cabo explained that “EN-PESA uses a machine learning algorithm called Elastic Net, which permits the unbiased analysis of a large number of variables. In this way, this system can identify new predictors not considered in established risk scores.” Moreover, EN-PESA treats the predictor variables quantitatively, “avoiding simplistic dichotomies such as ‘high cholesterol: yes/no’. This improves prediction and takes account of the specific characteristics of each individual to produce a personalized cardiovascular risk profile.”
The authors conclude that “this algorithm will improve the clinical management of apparently healthy individuals with a low cardiovascular risk according to established risk scores but who have a generalized extent of subclinical atherosclerosis or a high short-term risk of significant disease progression.”
Source: Read Full Article